Press Release – Female Athlete Triad: Double Check the Score
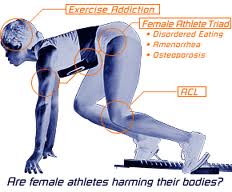
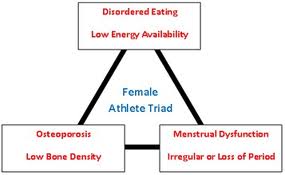
By Dr. Elizabeth Pilicy Girls who play soccer, or participate in any endurance sport, may be at risk to develop a combination of three disorders now commonly referred to as the "Female Athlete Triad." The female athlete triad is composed of the connected pattern of disordered eating, exercise-associated loss of normal cyclic menstrual periods (amenorrhea), and loss of bone mineral density or frank osteoporosis. This disorder is increasingly occurring in athletic women, particularly as more and more girls are participating in high level sports and are starting at increasingly younger ages. The inadequate nutrient supply to the body associated with disordered eating patterns is at the heart of this serious disorder. This triad as a whole often goes unrecognized. The consequences of lost bone mineral density can be devastating for the female athlete. Stress fractures or premature osteoporotic fractures can occur, and lost bone mineral density may never be regained.
Causes
Traditionally, this triad disorder has been considered a result of weight loss from a combination of high levels of training and low calorie consumption, particularly amongst females who are overly conscious of their weight. Studies now clearly demonstrate that the cause contributing most significantly to the female athlete triad, rather than merely a low body weight, is a negative calorie balance (more calories burned each day than ingested). Even exceedingly thin females who meet their energy requirements each day are protected from developing features of the triad. The individual components of the triad are further addressed below. Disordered Eating Disordered eating is a pattern of poor nutritional practices arising largely from poor food choices and a lack of knowledge about the importance of nutrition for fueling performance. This type of eating disorder plays a prominent role in generating a deficit of necessary nutrients for growth, development, and activity referred to as negative calorie balance. If athletic girls are overly concerned about body weight, their preoccupation with weight often leads to disordered eating behaviors. As an example, females may partake in meal skipping, overly exclusionary diets (protein predominant with low fat and minimal carbohydrate – which is absolutely contrary to a desirable intake pattern for an athlete), and excessive exercising to foster additional weight loss or compensate for the food that they have eaten. By disordered eating, that is to say the female is not ingesting or absorbing enough nutrients to support her body’s functions, thereafter affecting the natural pattern of the menstrual cycle as well as depleting the quality and density of the bones. Without proper nutrients, bones can not sustain sufficient bone maintenance for rebuilding and forming healthy bones. Amenorrhea Amenorrhea is defined as the absence of normal menstrual cycles. Primary amenorrhea is the failure to start having regular menstrual cycles while secondary amenorrhea is the cessation of previously established menstrual cycles. In the setting of physical stress such as calorie deficiency and high levels of physical training, the normal cyclic hormonal patterns in young ladies become disturbed or are completely disrupted. The most important of these is a relative deficiency in estrogen. Low levels of estrogen negatively influence the development and maintenance of bone mineral density in exercising girls. This is particularly important in light of the fact that young women can actively add to their bone density only until age 30-35. If they fail to establish strong bone health when young, they are at great risk to develop osteoporosis later in life. Osteoporosis Osteoporosis refers to abnormal loss of bone density resulting from a greater rate of bone breakdown than bone formation. This is a complex process, but in athletes the most important contributing factors to bone health are adequate intake of calcium and natural production of vitamin D, as well as hormonal balances. As such, female athletes who are estrogen deficient and nutritionally depleted because of poor eating habits are at great risk to develop bone thinning or even osteoporosis. The significance of this change in bone health has both short and long-term ramifications. During their athletic career, women with low bone density are at increased risk for sports-associated stress fractures. Later in life, low bone density at a young age predisposes to the development of frank osteoporosis, particularly after menopause. Bone density does respond favorably to weight-bearing exercise; consequently, many athletes feel that their training activities are sufficient to foster normal bone health. However, if the other factors of disordered eating and amenorrhea are present, weight-bearing exercise may not only fail to help bone density but may actually contribute to stress fractures. Screening/Diagnosis/Treatment Early recognition of the female athlete triad can be accomplished through risk factor assessment and screening questionnaires performed by a knowledgeable and qualified physician, such as a chiropractor. Increased education of parents, coaches and athletes in the health risks of the female athlete triad can prevent a potentially life-threatening illness. Thorough assessments may include a questionnaire, blood analysis, nutritional analysis assessing energy balance and nutrient balance. The physical examination of the athlete at risk for the Female Athlete Triad should focus on assessment of the physical signs of eating disorders and secondary signs of hormonal abnormalities. Comments are closed.
|
AuthorDr. Lizie Pilicy, Chiropractor and Nutritional Specialist, uses innovative holistic approaches to wellness incorporating mind, body, and spirit disciplines to assist with whole-being wellness. Categories
All
Archives
April 2024
|



 RSS Feed
RSS Feed
© 2024 Functional Health & Chiropractic Care. All rights reserved.
|
All information on our site is provided for information purposes only and does not constitute a legal contract between Dr. Lizie Pilicy and any person or entity unless otherwise specified. Although every reasonable effort is made to present current and accurate information, information is subject to change without prior notice. If you want to read through a bunch of legal jargon, here's our Privacy Policy and Terms of Use.
|
14330 Midway Road, Ste. 119
Farmers Branch, TX 75244 |